**
Overview
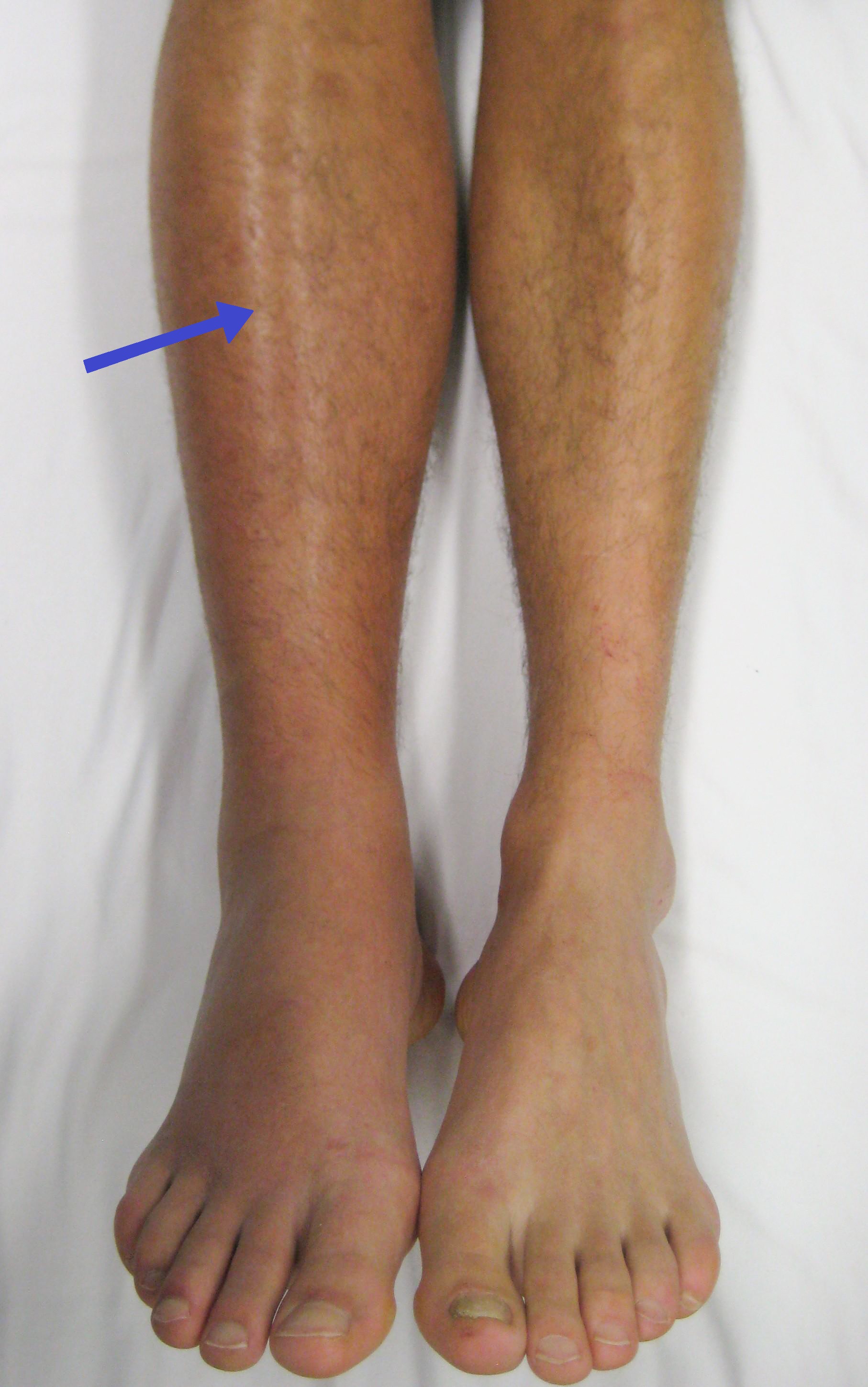
Deep vein thrombosis (DVT) refers to the formation of a thrombus (blood clot) within the deep venous system, typically of the lower extremities or pelvis. The clot can partially or completely obstruct venous outflow, leading to local symptoms such as pain, swelling, warmth, and visible superficial veins. However, up to one‑third of DVTs are clinically silent and are discovered incidentally on imaging performed for other reasons. The primary danger of DVT lies in its potential to dislodge; a fragment that travels to the lungs causes a pulmonary embolism (PE), a life‑threatening event that can result in sudden shortness of breath, chest pain, or cardiovascular collapse.Risk factors are broadly grouped into the classic Virchow’s triad: venous stasis (e.g., prolonged immobility, long‑haul travel), endothelial injury (e.g., surgery, trauma, intravenous catheters), and hypercoagulability (e.g., inherited clotting disorders, cancer, hormonal therapy). Age, obesity, smoking, and chronic inflammatory conditions also increase susceptibility. Diagnosis relies on a combination of clinical assessment (e.g., Wells score), D‑dimer testing, and definitive imaging—most commonly duplex ultrasonography. Treatment centers on rapid initiation of anticoagulation (heparin, low‑molecular‑weight heparin, or direct oral anticoagulants) to prevent clot propagation and embolization, followed by a tailored duration of therapy based on recurrence risk.
If you suspect you have a DVT, seek immediate medical attention. Prompt evaluation can prevent serious complications and guide appropriate therapy.
History/Background
The phenomenon of “blood clots in the leg” was first described in the mid‑19th century by French physician Jean‑Louis‑Alphonse Bégin, who linked post‑surgical leg swelling to thrombotic obstruction. In 1856, Rudolf Virchow articulated the three‑component model (stasis, injury, hypercoagulability) that still underpins modern understanding. The 20th century saw major advances: the introduction of heparin in the 1930s provided the first effective anticoagulant, while the development of warfarin in the 1950s enabled long‑term outpatient management. The 1990s ushered in low‑molecular‑weight heparins and, later, direct oral anticoagulants (DOACs), which simplified dosing and reduced monitoring requirements. Imaging breakthroughs, especially real‑time duplex ultrasound (1970s) and CT pulmonary angiography (1990s), transformed diagnostic accuracy and allowed earlier detection of both DVT and PE.Key Information
- Epidemiology: Approximately 1–2 per 1,000 persons develop DVT each year; incidence rises sharply after age 60. - Common sites: Popliteal, femoral, and iliac veins; upper‑extremity DVT accounts for <10 % of cases and is often catheter‑related. - Symptoms: Unilateral calf pain, swelling, erythema, and a feeling of heaviness; “Homan’s sign” (pain on forced dorsiflexion) is unreliable. - Diagnostic tools: Wells clinical prediction rule, high‑sensitivity D‑dimer, compression duplex ultrasonography; venography is reserved for equivocal cases. - Management: Immediate anticoagulation (LMWH, UFH, or DOAC), compression stockings to reduce post‑thrombotic syndrome, and in selected patients, catheter‑directed thrombolysis or vena cava filter placement. - Duration of therapy: Typically 3 months for provoked DVT; extended or indefinite anticoagulation is considered for unprovoked or recurrent events, or in the presence of persistent risk factors. - Complications: Pulmonary embolism (mortality up to 15 % if untreated), post‑thrombotic syndrome (chronic pain, edema, ulceration), and recurrent thrombosis.Significance
DVT is a major public health concern because of its frequency, potential for fatal embolic events, and long‑term morbidity. It is a leading cause of preventable hospital‑acquired complications, prompting widespread implementation of prophylactic protocols (e.g., pharmacologic agents, mechanical compression devices) in surgical and medical in‑patient settings. Economically, DVT and its sequelae generate billions of dollars in healthcare costs annually, driven by hospitalizations, imaging, anticoagulant therapy, and management of chronic complications. The evolution of DOACs has markedly improved patient adherence and reduced routine laboratory monitoring, reshaping outpatient care models. Ongoing research into genetic risk profiling, novel antithrombotic agents, and personalized duration of therapy continues to refine risk‑benefit balances, aiming to lower both clot recurrence and bleeding complications.INFOBOX:
- Name: Deep Vein Thrombosis
- Type: Venous thromboembolic disease
- Date: First clinical description mid‑19th century (≈1850)
- Location: Deep veins of lower extremities, pelvis; occasional upper‑extremity involvement
- Known For: Formation of clot in deep veins with risk of pulmonary embolism
TAGS: deep vein thrombosis, venous thromboembolism, anticoagulation, pulmonary embolism, thrombosis risk factors, duplex ultrasonography, post‑thrombotic syndrome, vascular medicine



