Overview
Kidney cancer refers to a heterogeneous group of malignancies that arise from the renal parenchyma, the functional tissue of the kidney. The most common subtype is renal cell carcinoma (RCC), accounting for about 85 % of adult cases, while transitional cell carcinoma of the renal pelvis and Wilms tumor in children represent less common forms. Typical presentations include hematuria (blood in the urine), a palpable abdominal mass, and flank or back pain. Systemic symptoms such as fever, unexplained weight loss, and fatigue may also occur, reflecting the tumor’s metabolic activity or paraneoplastic phenomena.Diagnosis usually begins with imaging—ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI)—to visualize the lesion, followed by a percutaneous needle biopsy when the imaging is inconclusive. Staging relies on the TNM system (Tumor size, Node involvement, Metastasis) and guides treatment decisions. Early-stage disease (confined to the kidney) often allows for curative surgery, whereas advanced disease may require systemic therapies, including targeted agents, immunotherapy, or clinical trial enrollment. Prompt evaluation by a healthcare professional is essential; anyone experiencing persistent hematuria, unexplained pain, or systemic symptoms should seek medical attention.
History/Background
The first recorded description of kidney tumors dates back to the 19th century, when pathologists noted “cancer of the kidney” in autopsy reports. In 1895, Friedrich von Recklinghausen distinguished renal carcinoma from other abdominal neoplasms based on histology. The mid‑20th century saw the development of radical nephrectomy (removal of the entire kidney, adrenal gland, and surrounding tissue) as the standard surgical cure, pioneered by William J. Mayo and colleagues. The 1980s introduced partial nephrectomy, preserving healthy renal tissue for small tumors, a shift driven by advances in imaging and surgical techniques.A major breakthrough occurred in the early 2000s with the discovery of the von Hippel‑Lindau (VHL) gene and its role in RCC pathogenesis, leading to the first targeted therapies (e.g., sunitinib, sorafenib) that inhibit angiogenesis. More recently, immune checkpoint inhibitors such as nivolumab have transformed the treatment landscape for metastatic disease, offering durable responses for a subset of patients. Ongoing research into genomics, biomarkers, and combination regimens continues to refine personalized care.
Key Information
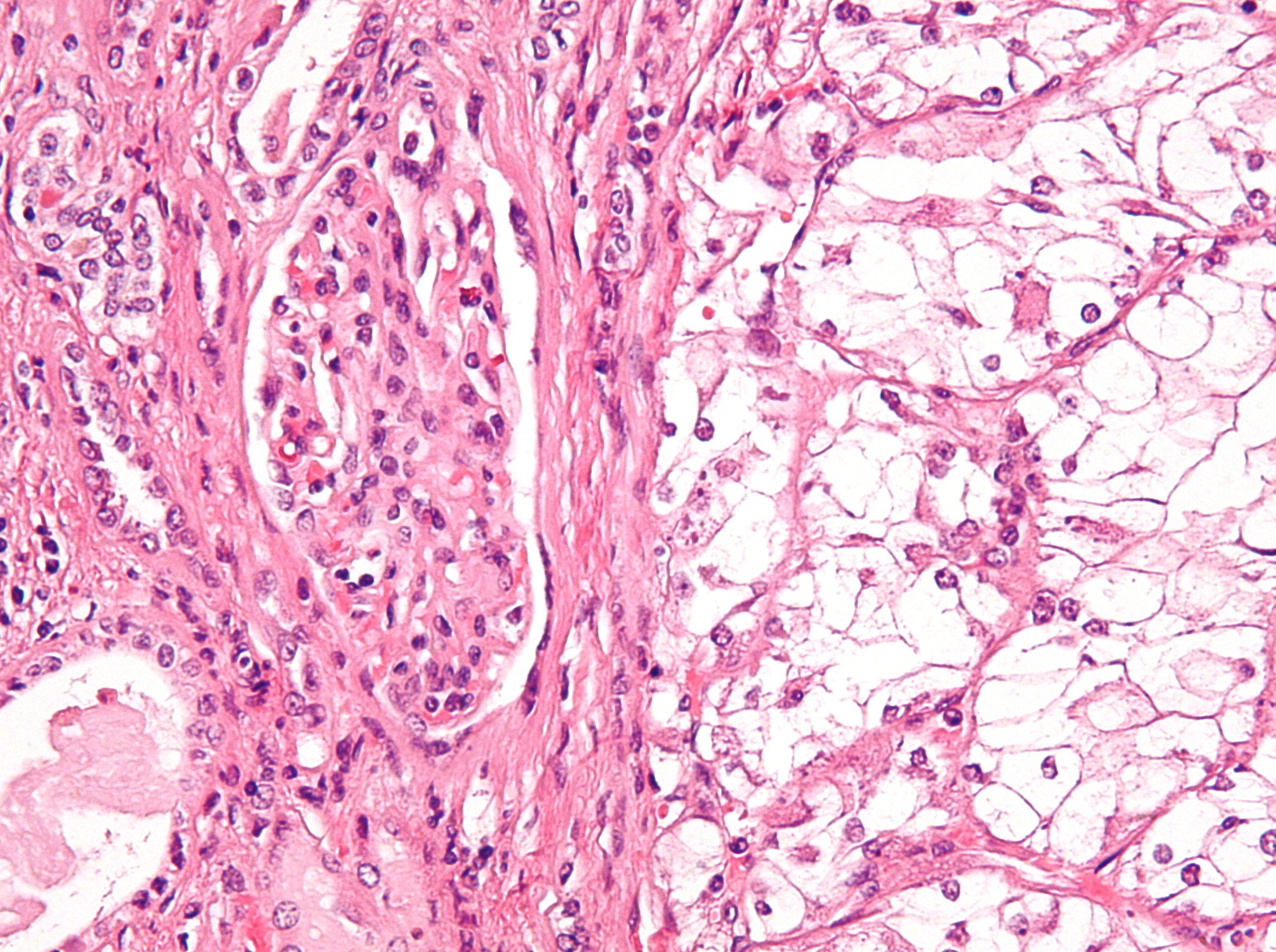
- Epidemiology: Kidney cancer is the 9th most common cancer worldwide, with an estimated 430,000 new cases and 180,000 deaths annually (2023 data). Incidence is higher in men (≈1.5 × women) and peaks between ages 60–70. Major risk factors include smoking, obesity, hypertension, chronic kidney disease, and occupational exposure to certain chemicals (e.g., trichloroethylene). - Pathology: RCC subtypes include clear‑cell (≈75 % of cases), papillary, chromophobe, and collecting‑duct carcinoma, each with distinct genetic alterations. Clear‑cell RCC is strongly linked to VHL loss, leading to overproduction of vascular endothelial growth factor (VEGF). - Diagnosis: Initial work‑up comprises urinalysis, serum creatinine, and imaging. Contrast‑enhanced CT is the gold standard for characterizing tumor size, vascular involvement, and metastatic spread. Biopsy is reserved for atypical lesions or when non‑surgical management is contemplated. - Staging & Prognosis: The TNM stage correlates with 5‑year survival: Stage I (localized) ≈ 90 %, Stage III (regional spread) ≈ 60 %, Stage IV (distant metastasis) ≈ 12 %. Prognostic models (e.g., MSKCC, IMDC) incorporate clinical variables such as performance status, hemoglobin, calcium, and time from diagnosis to treatment. - Treatment: - Localized disease: Partial or radical nephrectomy (open, laparoscopic, or robotic). Ablative techniques (radiofrequency, cryoablation) are options for small (<4 cm) tumors in patients unsuitable for surgery. - Advanced/metastatic disease: First‑line regimens often combine a VEGF‑targeted tyrosine kinase inhibitor (TKI) with an immune checkpoint inhibitor. Subsequent lines may include alternative TKIs, mTOR inhibitors, or enrollment in clinical trials. - Complications: Metastatic spread commonly involves the lungs (≈ 50 % of cases) and brain (≈ 10 %). Paraneoplastic syndromes—hypercalcemia, erythrocytosis, hypertension—can complicate management.When to seek professional care: Persistent blood in the urine, unexplained flank pain, a new abdominal lump, or systemic symptoms such as fever and weight loss warrant prompt evaluation by a physician. Early detection improves treatment options and outcomes.



