**
Overview
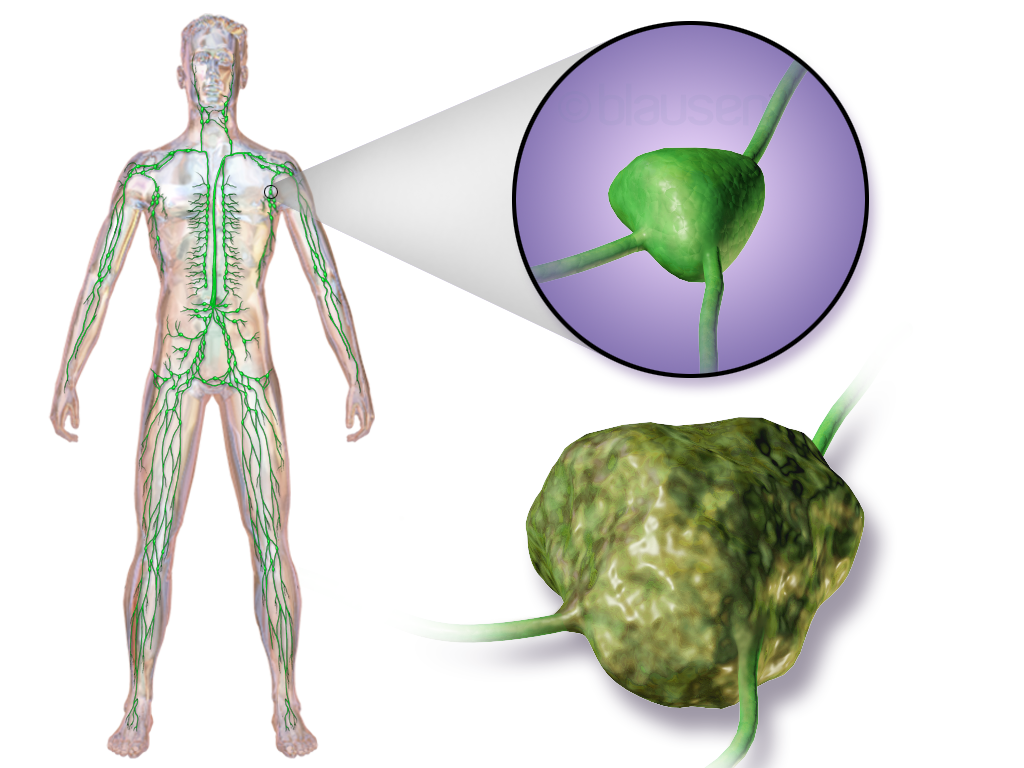
Lymphoma encompasses a heterogeneous collection of blood and lymphatic system tumors that originate from B‑cells or T‑cells, the two main types of lymphocytes. Although the term “lymphoma” can technically describe any abnormal growth of lymphoid tissue, in clinical practice it is reserved for the cancerous forms that spread through the lymphatic network, blood, and sometimes other organs. The disease is broadly divided into Hodgkin lymphoma (HL), characterized by the presence of Reed‑Sternberg cells, and non‑Hodgkin lymphoma (NHL), a diverse group that accounts for roughly 85 % of all cases.
Patients often present with painless, enlarged lymph nodes, most commonly in the neck, armpits, or groin. Systemic “B‑symptoms”—fever, drenching night sweats, and unintended weight loss—signal a more aggressive disease course. Additional complaints may include pruritus (itching), persistent fatigue, and, in advanced stages, organ‑specific symptoms such as abdominal pain from splenomegaly or shortness of breath from mediastinal masses. Because early signs can mimic benign infections, a high index of suspicion and prompt diagnostic work‑up are essential.
History/Background
The first documented description of a lymphoma‑like disease dates to 1845, when Thomas Hodgkin reported a case of “a disease of the lymphatic system” in a young man with enlarged cervical nodes. The eponymous Hodgkin lymphoma was formally named after him in the early 20th century. In the 1950s, the Rappaport classification introduced a histologic framework that distinguished between Hodgkin and non‑Hodgkin types, paving the way for modern taxonomy. The 1970s and 1980s saw the advent of combination chemotherapy (e.g., CHOP) and the first monoclonal antibody therapy (rituximab) for B‑cell NHL, dramatically improving survival. Ongoing research into genomic profiling and immune checkpoint inhibition continues to refine treatment paradigms.Key Information
- Epidemiology: Approximately 9 % of all cancers worldwide are lymphomas, with an incidence of ~5 per 100,000 persons annually in high‑income nations. HL shows a bimodal age distribution (young adults and >55 years), whereas NHL incidence rises steadily with age. - Risk Factors: Immunosuppression (HIV, organ transplantation), chronic infections (EBV, H. pylori, HTLV‑1), certain autoimmune diseases, and exposure to chemicals (pesticides, benzene) increase risk. - Diagnosis: Core components include excisional lymph node biopsy, immunophenotyping (flow cytometry), cytogenetic studies, and imaging (PET‑CT). Staging follows the Ann Ann Arbor system, incorporating the number of involved sites and presence of B‑symptoms. - Treatment: Therapeutic strategies are tailored to subtype, stage, and patient factors. First‑line regimens range from ABVD for early‑stage HL to R‑CHOP for many B‑cell NHLs. Advanced or refractory disease may require high‑dose chemotherapy with autologous stem‑cell rescue, CAR‑T cell therapy, or immune checkpoint inhibitors (e.g., pembrolizumab). - Prognosis: Five‑year survival exceeds 85 % for early‑stage HL but varies widely for NHL (from >90 % for indolent follicular lymphoma to <30 % for aggressive peripheral T‑cell lymphomas).When to seek professional care: Any persistent, painless swelling of lymph nodes lasting more than two weeks, unexplained fever, night sweats, weight loss, or ongoing fatigue warrants evaluation by a healthcare professional. Early diagnosis improves treatment options and outcomes.
Significance
Lymphoma’s impact extends beyond individual patients; it drives advances in cancer biology, immunology, and targeted therapy. The success of rituximab, the first monoclonal antibody approved for cancer, sparked a wave of biologic agents now standard across oncology. Moreover, lymphoma research has illuminated mechanisms of immune evasion, informing the development of checkpoint inhibitors that benefit a broad spectrum of malignancies. From a public‑health perspective, survivorship programs address long‑term effects such as secondary malignancies, cardiovascular disease, and psychosocial challenges, underscoring the need for comprehensive, multidisciplinary care.INFOBOX:
- Name: Lymphoma (Hodgkin and Non‑Hodgkin)
- Type: Malignant neoplasm of lymphoid tissue
- Date: First described 1845 (Hodgkin’s disease)
- Location: Primarily lymph nodes; may involve spleen, bone marrow, extranodal sites
- Known For: Pioneering use of monoclonal antibodies and CAR‑T cell therapy in cancer treatment
TAGS: lymphoma, Hodgkin lymphoma, non‑Hodgkin lymphoma, oncology, immunotherapy, chemotherapy, hematology, cancer research



